Everyone agrees that not all Ankle Foot Orthoses (AFOs) are the same and they do not treat the same pathologies. Also different designs have varying effects on biomechanical function. However, the terms used to describe the different types of AFOs have not been fully classified and defined. This has led to the use of varying descriptions and acronyms resulting in poorly designed research studies (1,2) and a misunderstanding of research outcomes. The lack of classification has also resulted in generalisation on the effects of AFOs from research studies which have not been clear on the design of the AFO used or the presenting pathology it was used for (2), with some studies describing the AFO as “a standard AFO”, for which there is no definition. Standardised terminology and definitions for AFOs are critical in clinical practice, without these, there may be serious negative consequences, with the potential to cause harm.
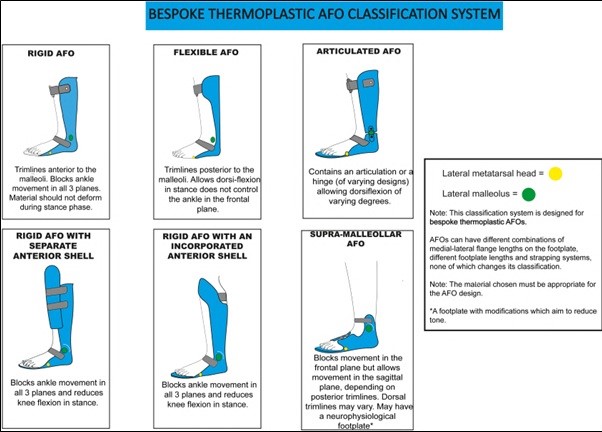
We have now developed and validated a new classification system for different designs of bespoke thermoplastic AFOs.
Figure 1: Bespoke thermoplastic AFO classification chart.
The proposed classification system for bespoke thermoplastic AFOs, has an excellent inter- and intra-observer agreement. It will reduce the ambiguity of the description of the type of AFOs used in clinical practice and research. Furthermore, it makes reproducible comparisons between groups possible, which are essential for future evaluations of evidence-based orthotic care.
Figueiredo EM, Ferreira GB, Maia Moreira RC, Kirkwood RN, Fetters L, Figueiredo E, Ferreira G, Moreira R, Kirkwood R FL. Efficacy of Ankle-Foot Orthoses on Gait of Children with Cerebral Palsy: Systematic Review of Literature. Pediatr Phys Ther. 2008;20(3):207-223. doi:10.1097/PEP.0b013e318181fb34
Eddison N, Mulholland M, Chockalingam N. Do research papers provide enough information on design and material used in ankle foot orthoses for children with cerebral palsy? A systematic review. J Child Orthop. Published online July 3, 2017:1-9. doi:10.1302/1863-2548.11.160256
Footwear advice created from footwear assessment is often anecdotal based on individual clinical experience and interest. There is often no structured way to evaluate the shoe worn to clinic and a generalised opinion on footwear choice is given.
Isolated assessment of footwear can provide a number of challenges for clinicians as wider footwear choices made by patients often do not reflect the shoes worn to appointments. This creates an unrealistic view for the clinician and inaccurate assumptions are often made when issuing advice.
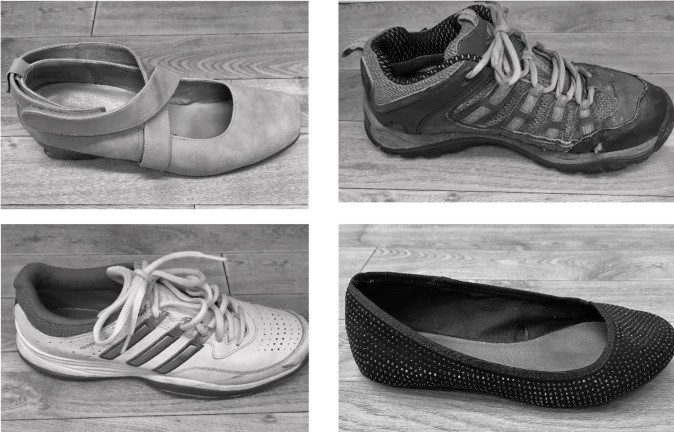
To assist clinicians in assessing shoes we have developed a simple valid clinical footwear tool.
This tool has been designed to help clinicians quantify and measure a full range of footwear in one appointment. The footwear tool also provides a systematic view to assess the quality of fit and design of the shoe whilst channelling the clinician towards developing individual footwear advice for the patient. The tool is multifaceted and addresses a number of parameters associated with good fit and footwear choice.
Our validation of the tool shows that it is reliable to use in the clinic and can be applied to a number of styles of shoes. There is minimal equipment required to use the tool and completion of the assessment takes a short period of time.
The COVID-19 pandemic saw an unprecedented expansion of telehealth with a shift to remote patient consultations across the allied health professions.
Our study published in BMJ Open has examined current guidelines for the 14 Allied Health Professionals (AHPs) in the UK reveals a clear need to solve the disparities in the level of guidance for remote consultations between professions.
While telehealth can be considered an efficient and safe way to deliver consultations, in practice there are barriers which can lead to unintended consequences; these include technological constraints such as inadequate internet bandwidth, lack of skills among users, patient confidentiality, privacy as well as data security issues.
Additionally, concerns have been raised about the risk of patient harm resulting from the lack of diagnostic and therapeutic quality of services delivered through telehealth, as this can lead to highly infectious and life-threatening conditions being missed.
The study revealed that most telehealth guidelines were designed to quickly respond to the need for remote patient consultations during the Covid-19 pandemic and recommends that available guidelines should be reviewed to ensure they meet the long-term needs of patient consultations.
Very few guidelines were specifically designed for certain clinical populations, which acknowledged that telehealth consultations need to be adapted to meet individual needs. It was also found that most guidelines were specifically designed for occupational therapists, physiotherapists and speech and language therapists, leaving the other AHP groups with very few or inadequate guidelines.
Everyone has a right to certain products and devices that can help them function in everyday life. This is the stance of the World Health Organisation (WHO), which has published a list of the most important of these devices. It includes things like walking aids, wheelchairs and braille displays.
But assistive technologies, as they are called, are difficult to access in many parts of Africa. This is a huge problem because the prevalence of disabilities on the continent is estimated at 15.6%. With a population of more than one billion, the number of people in need of at least one assistive product in Africa stands at over 200 million, and that figure is projected to double by 2050.
The WHO estimates that only about 15% to 25% of those in need of assistive technology products in Africa currently have access to them.
Our research sought to find out why and to offer solutions to this problem.
Human rights
Assistive technologies are functional, adaptive, and rehabilitative devices. Not only does the WHO support a global commitment to making them more easily available, the United Nations also regards them as a basic human right. This is because some people need them in order to exercise their rights.
Without access to the assistive technology they need, people can face exclusion and are at risk of poverty. They may also be perceived as a burden to their families and society. The positive impact of assistive technology products goes far beyond improving the health and well-being of users. There are also the socio-economic benefits of reducing direct health costs and having a more productive labour force, indirectly stimulating economic growth.
The 2006 UN Convention on the Rights of Persons with Disabilities and its optional protocol was negotiated quickly and well supported by member states. It was also the first human rights convention to be open for signature by regional integration organisations. But its implementation has been shaky, particularly in Africa.
We believe this is best explained by the idea of economic and political institutional voids. These are basically gaps in political and economic systems, trade policies and markets. An absence of specialised intermediaries, regulatory systems and contract enforcing mechanisms creates higher transaction costs for doing business or even entering markets.
Seeing the problem in this way also helps to show how to solve it and achieve fair access to assistive technologies.
Institutional voids
First, there is little production of assistive technologies in Africa because the parts are generally expensive to make. Many indigenous producers use crude and unstandardised materials.
Second, assistive technologies that are not produced locally are expensive to import. There are no unified tariff structures for them within the continent. This means that costs vary widely from country to country. Often, when assistive technologies do get imported despite high tariffs, they might need to be adapted for the local environment. This increases the costs even further.
Third, assistive technologies are mostly excluded from health financing and insurance schemes on the continent. They are not often included in central medical store catalogues.
Fourth, there aren’t enough people at all levels of the health system with the required knowledge and skills to provide assistive technology services and products.
Fifth, and most crucially, there is no unified governance framework for assistive technologies on the continent. And there’s a widespread lack of awareness about why they are needed and how they can improve the lives of people who need them.
Most African countries do not have national assistive technology policies or programmes. As a result, access to assistive products is difficult and many are left behind.
Solutions
African governments need to provide leadership, coordination and resources to plan and implement policies that increase access to assistive technologies.
Acting on the WHO African regional framework is a good place to start. The framework has modest aims. For instance, it calls for 40% of African member states to have assessed their assistive technology situation and developed a national strategy to improve access by 2024. This will help 40% of the population in Africa that needs assistive products to get them without suffering financial hardship.
The African Union can learn from the European Union. The European Parliamentary Research Service has commissioned and published an in-depth report of assistive technologies. The report covers economic, political and socio-ethical perspectives and it tries to implement the declarations that assistive technologies are a basic human right. Such a focused and thorough evaluation is missing in Africa.
To produce technologies on the continent, the African Union should develop a market strategy. The current market is one where the players are left to fend for themselves, and so face high operating costs. These costs ultimately make assistive technologies expensive.
Producers should also embrace frugal innovation – the process of reducing the complexity and cost of an item and its production, usually by removing nonessential features.
Qualified personnel are another part of the solution.
Finally, but maybe most importantly, there is a need for a structured enquiry to highlight the gaps in economic, political, scientific, and clinical knowledge for assistive technology development and deployment in Africa – and a unified approach to solving the problems.
This would help millions of people in Africa to achieve their basic rights such as access to education, freedom to live, and the right to work.
Our recent paper has established recognised terms, definitions, design characteristics and prescription criteria for off-the-shelf stability footwear for the first time.
Numerous terms have been used in the literature concerning clinical footwear interventions, including orthopaedic shoes, rehabilitative boots, modified shoes, supportive shoes and special shoes. There is also no standardised set of agreed outcome measures, both physical and psychosocial, to ascertain the effectiveness of this footwear.
A group of multinational professionals, from clinicians to those involved in the footwear industry, were recruited to take part in an online survey and to provide further insights through a series of open-ended questions.
“Therapeutic footwear” was the agreed term to represent children’s footwear interventions, with grouping and subgrouping of therapeutic footwear being dependent on their intended clinical outcomes: accommodative, corrective or functional. Design characteristics of off-the-shelf footwear were also grouped under three themes: stability, ergonomics and aesthetics.
This is believed to have many benefits including:
A common understanding of therapeutic footwear terminology to facilitate communication between clinicians, researchers and manufacturers.
Research-informed evidence for selection of appropriate off-the-shelf stability therapeutic footwear based on identified design characteristics.
Research-informed evidence for dispensing off-the-shelf stability therapeutic footwear to patients.
Standardised outcome measures for clinical assessment of the effectiveness of off-the-shelf stability therapeutic footwear interventions.
This study has achieved an expert consensus where none previously existed, which is important from both a manufacturing and clinical perspective. This is a huge step forward which we hope will lead to quicker, more personalised and more effective treatment for children with mobility issues.
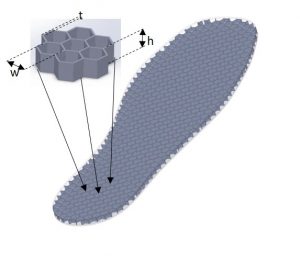
We have developed a novel concept to assess plantar laoding using 3D-printed, tuneable structures. This will help clinicians better understand the cause of foot ulcer development in patients with diabetes and lead to improved clincal outcomes.
Dr Chatzistergos, who led the study, said: “Our work has demonstrated a method to reliably detect overloading using a low-cost non-electronic technique. We have used a 3D-printed thin-wall structure that changes its properties when repeatedly loaded above or below a tuneable threshold. We believe that this is a step change from current practice.”
This year, Children’s Wisconsin and their academic partners, The Medical College of Wisconsin, were the hosts for the 2021 International Research Society for Spinal Disorders conference.
The Society was founded in 1992 with the tenet to integrate basic science with clinical care to benefit patients from across around the world. IRSSD conferences provide interaction between clinicians and researchers with interests in spinal biomechanics, imaging and measurement, genetics aetiopathogenesis, growth and metabolism, innovations in conservative and surgical therapies, and quality of life and functional outcomes, to mention just some of the areas of activity.
The pandemic de-railed the physical conference with just short of 200 attendees spent a fascinating, insightful, and very well run virtual event in late January. Professor Nachi Chockalingam, Dr Rob Needham, and Professor Tom Shannon presented work and opinion within a symposium entitled Gait and Posture Analysis in Scoliosis-Implications for Clinical Practice, with Dr Ram Haddas from the Texas Back Institute. After the presentations, Nachi hosted a very lively and interesting questions session.
Nachi, Tom and Nikola Jevtić from the Scolio Centar, Novi Sad, Serbia presented our work inCosmetic changes in patients following a Schroth Exercise Regime: a two year follow-up.The primary objective of our longitudinal study has been to investigate the relationship between scoliosis spinal deformity measures, clinic reports, images, curve classifications, and back shape data with the goal to develop, test and validate some new cosmetic deformity metrics. Our work is starting to show encouraging results, and we were hugely honoured to be awarded one of the two poster prizes.
This exciting work continues in Serbia and Bulgaria with donated equipment now also installed in Banja Luka, Bosnia and Herzegovina to expand the research efforts in that country as well.
Our latest paper published in the BMJ Open highlight large variances in appointment times, waiting times, product entitlements for patients, and product lead times across various NHS trusts.
Although some geographical areas provide shorter waiting times and wider access to assistive devices, other areas have very long waiting time which means that the service, particularly to the paediatric population is meaningless.
The NHS trusts seemed to be able to answer questions that reflect quantity of service above quality of service. However, the combination of the number of Trusts who declined to reply to the FOI request and those who replied with limited information, hindered the ability of this study to collate the data received to provide a fuller national picture of the Orthotic Service provision.
Although this paper confirms that many of the issues reported in previous reports on Orthotic Service provision are still evident, the result show that there have been some improvements.
The decision of where to study for a master’s degree was a difficult one. There seemed to be an endless choice of institutions, with a multitude of differing delivery models. I was working as a podiatrist and an undergraduate lecturer, I had both teaching and clinical commitments which I couldn’t escape for long periods and the idea of a purely online course seemed tempting; however, deep down I knew that work and life pressures would likely mean my studies may take a back seat. The MSc Clinical Podiatric Biomechanics course seemed ideal, the teaching was blended taught sessions on a weekend, so my day job didn’t need to suffer and there was online support available. This was a bonus as I live in the North East of England and the idea of popping in for a quick tutorial wasn’t possible.
The course was delivered by excellent teaching staff, people who were not only passionate about the subjects they specialised in, but were the authors of the current literature which I had been reading to develop my own clinical practice. In all honesty I was a little star struck, when I met some of them. I was determined not ask a “stupid question”, however, every tutor made me feel at ease and provide a safe and supportive environment which meant there were no “stupid questions”. The discussions that formed were insightful and helpful, led by the tutor guiding us to through the subject. This learning experience is one I have never encountered before and is one I try to model within any teaching sessions I deliver.
The support continued throughout my time studying with Staffordshire University, all my tutors were on hand with a quick reply to an email or to arrange a time for a telephone call which, they managed to fit around my working schedule. This support never wavered even when I started my dissertation. I had excellent guidance from day one; I had opportunity to spend time discussing with my supervisor my research idea, developing my methodology and setting a realistic time frame. At my first meeting my wife was 6 months pregnant with our 1st child. My tutor helped me set a timetable and deadlines which were achievable. Without this I feel, I would have made this process almost impossible for myself and possibly not finished at all. Balancing the demands to complete a research project, write a thesis and live with a new born was challenging. But my tutor had an excellent skill to allow me the space to progress and work, but check in exactly when I needed a boost, some encouragement or just the opportunity to share where I was up to. I completed my project and received a good grade; I was so proud of my achievement through whole duration of my study and felt I had completed a well-rounded piece of research. I have to admit I was surprised when my tutor suggested that I should publish my research. I had never published in a scientific journal, “that’s the sort of thing experts do” I thought. However, as I reflected, I realised that my research was worthy of publication. I had no idea where to start, but my tutors came to my rescue again providing me with the same level of support I had before ( For people who are interested in reading our work, please follow this link).
I am so glad I chose to study with Staffordshire University and the teaching team on MSc Clinical Biomechanics course. I have not only gained a qualification, but published researched, developed a professional network that are always happy to share and discuss learning and most importantly I have developed as clinician. It has not only helped my practice and patients but the experience has allowed me to grow as a professional.
Branthwaite, H., Aitkins, C., Lindley, S. and Chockalingam, N., 2019. Surface Electromyography of the foot: a protocol for sensor placement. The Foot. https://doi.org/10.1016/j.foot.2019.07.001
One of our classic papers looked at the influence of practitioners and their skills in prescribing foot orthosis which are commonly prescribed and used in treating numerous lower limb problems.
Over the years several studies have reported positive effects and most clinical practitioners would confirm those findings. However, the exact mechanisms in which these orthoses work are not fully understood.
Our results suggest that the type and amount of effects observed is greatly influenced by the practitioners. From a scientific perspective, this indicates that great caution should be taken when studying and reporting the effects of custom foot orthoses (CFO). Had only one practitioner been used for studying CFO effects on kinematics, altogether different conclusions could have been drawn based on a single pair of CFO.
We recommend that future research on foot orthoses should focus on their long-term effect through longitudinal studies. Nevertheless, based on the reported data, it seems improbable that two different devices could yield the exact same results.
Most CFO will induce some systematic changes during gait. Furthermore, this study demonstrated that inter-practitioner variability is a major factor in orthotic intervention in treating a single patient and for a specific pathology. Based on the findings, it is strongly recommended to use caution when drawing general conclusions from research studies using CFO as it has been showed that the practitioner himself or herself will have a great influence on the treatment outcome. In addition, comparing studies on CFO where different practitioners were involved should be done with great caution as the conclusion could vastly differ.
Reference:
Chevalier, T.L. and Chockalingam, N., 2012. Effects of foot orthoses: how important is the practitioner?. Gait & posture, 35(3), pp.383-388.




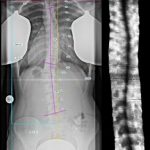
 The primary objective of our longitudinal study has been to investigate the relationship between scoliosis spinal deformity measures, clinic reports, images, curve classifications, and back shape data with the goal to develop, test and validate some new cosmetic deformity metrics. Our work is starting to show encouraging results, and we were hugely honoured to be awarded one of the two poster prizes.
The primary objective of our longitudinal study has been to investigate the relationship between scoliosis spinal deformity measures, clinic reports, images, curve classifications, and back shape data with the goal to develop, test and validate some new cosmetic deformity metrics. Our work is starting to show encouraging results, and we were hugely honoured to be awarded one of the two poster prizes. to expand the research efforts in that country as well.
to expand the research efforts in that country as well.